
There are many injuries that forced athletes out of training or competition, some injuries more than others. An injury that can become problematic over time are meniscus tears. It is well known that the knees are a common site of injury in all sports, and overall the American Academy of Orthopedic Surgeons estimate that they perform 850,000 meniscectomies per year (1).

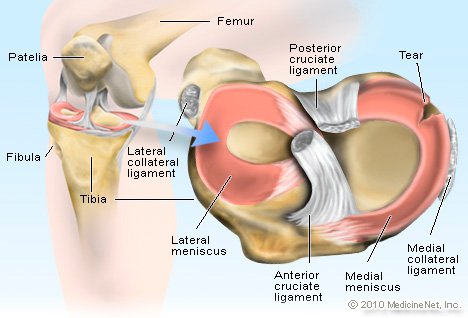
The menisci are fibrocartilaginous structures located in the knee joint. These wedge shaped structures play an important role in knee joint stability and biomechanics, they transmit anywhere from 50-90% of compressive forces depending on the angle of the knee joint. The menisci are our shock absorbers, they endure compressive, shearing, tensile forces on a daily basis. Therefore, the more active you are the more stress these structures encounter, the more degeneration they will undergo and in some cases may suffer from small to large tears.
The lateral meniscus is O-shaped while the medial meniscus is more C-shaped and unfortunately the whole structure is not well vascularized. The periphery of the menisci receive the most blood supply while the most central portion receive none. Due to this, tears that extend into the inner portion of the menisci have a very difficult time healing and therefore tend to not be repaired.
Most meniscus injuries involve the medial meniscus mostly because it is more fixed, it attaches to the joint capsule and medial collateral ligament of the knee (MCL).
A recent study specifically looked at the rate of meniscus injury in long distance runner and found that there was a slightly higher occurrence of meniscal lesions in higher trained runners vs lower trained runners (7), which has deduced to be to higher loads and increases in repetitive stresses. Most runners who suffer from a meniscus injury will be considered a "degenerative meniscus tear/injury." Acute tears in runners will most often be seen in trail runners where they have landed on a rock wrong and twist their knee, track runners who have been tripped on the track, or hurdlers who have landed wrong.
Mechanism of Injury
A majority of articular cartilage lesions result from trauma or repetitive minor trauma. In most cases a tear occurs a s a result of twisting the knee while the foot is planted (there is load on the leg). This can occur with a sudden turn or change in direction.
According to research the risk factors to developing acute meniscal tears are (6):
1. Sports: soccer, rubgy, running
2. Weight bearing during trauma
3. Increased BMI

The most common tears are vertical longitudinal, oblique, degenerative, and radial, and horizontal.
Signs and Symptoms:
1. Pain with bending, walking, exercising on the inside or outside of the knee
2. Swelling
3. Locking (if the tear is severe enough)
4. Catching
5. Clicking that is painful
Management:
What guides medical professionals to the intervention is based on symptoms severity, disability, and extent of injury.
Indications for a meniscus repair are as follows:
1. Meniscus tear with tibiofemoral joint line pain
2. Patients younger than 50 y.o , or >50 but athletically active
3. Concurrent knee ligament reconstruction
4. Reducible meniscal tear, good tissue integrity, normal joint like position post surgery
5. Peripheral single longitudinal tear
6. Middle third region tear with some vascularity
If surgery in contra- indicated conservative treatment is sought after, which consist of pain management and physical therapy. The rehabilitation program consist of:
1. Normalizing knee active and passive range of motion.
2. Normalization muscle imbalance of the muscle above and below the knee joint
3. Improving movement impairments
4. Steady progression of strength and function.
Meniscus injury outcomes :
For the individuals and undergo surgery about 80% of athletes will return to original sport (5). According to the literature the athletes who are under 40 y.o, have suffered an acute and painful tear and have symptoms of locking and catching have a success rate of 8% to return to sport after surgery. For the individuals suffering from degenerative meniscal injuries conservative treatment is always considered first. Surgery for degenerative meniscal injuries have a low success rate of 50% return to sport.
My personal thought on meniscus tears is:
1. If there was a trauma and injured your knee, you can't play your sport and its a an acutely diagnoses meniscus tear- repair it, rehab, and get back out there.
2. If not: REHAB, CHANGE THE WAY YOU MOVE, OPTIMIZE MUSCLE FUNCTION, BE PATIENT AND YOU WILL GET BACK.
TRAIN SMART
JESSICA MENA PT, DPT, OCS, CSCS
Doctor of Physical Therapy
Board Certified Orthopedic Clinical Specialist
Certified Strength and Conditioning Specialist

References:
1. Baumgarted B. To Run or Not to Run: A Post-Menisectomy Qualitative Risk Analysis Model for Osteoarthritis When Considering a Return to Recreational Running. Journal of Manual Therapy. 2007. 15(1)
2. Cavanaugh JT, Killian SE. Rehabilitation Following Meniscal Repair. Current Rev. Musculoskeletal Medicine. 2012 5(1).
3. Gray JC. Neural and Vascular Anatomy of the Menisci of the Human Knee. Journal of Orthopaedic and Sports Physical Therapy. 1999 29. (1).
4. Logerstedt DS, Scalzitti DA, Bennell KL, Hinman RS, Granelli HS, Ebert J, Hambly K, Carey JL, Mackler LS, Axe MJ, McDonough CM. Knee Pain and Mobility: Meniscal and Asticular Cartilage Lesions Revision 2018. Clinical Practice Guidelines.
5. Nakayama H, Kanto R, Kambara S, Kurosaka K, Onishi S, Yoshiya S, Yamaguchi M. Clinical outcome of the meniscus repairfor isolated meniscus tear in athletes. Asia-Pacific Journal of Sports Medicine, Arthroscopy, Rehabilitation Technology. 2017 10(4)
6. Snoeker BA, Bakeer EW, Kegel CA, Lucas C. Risk Factors for Meniscal Tears: A Systematic Review Including Meta- Analysis. Journal of Orthopaedic and Sports Physical Therapy. 2013. 43(6).
7. Weidekamm-Schueller C. Schueller G, Uffman M, Basder T. Incidence of Chronic Knee Lesions in Long-Distance Runners based on training level: Findings at MRI. European Journal of Radiology. 2006. (58).